
 Hunting African Big Game Hunting
Hunting African Big Game Hunting Go | New | Find | Notify | Tools | Reply |
| How to Prevent and Treat Malaria -- Brought to you by Global Rescue | Login/Join |
| One of Us |
April 25 is World Malaria Day. Malaria is found most often in Africa, Southern Asia, Central America, and South America, and is relatively rare in the United States. Malaria is caused by a bite from a parasite-infected mosquito. Symptoms of malaria can include fever, chills, sweats, body aches, and muscle pain. Fever that goes away and comes back is fairly common. Nausea, vomiting, abdominal pain, backache, and dark urine are also possible symptoms. More severe forms involving altered mental status and organ involvement typically require hospitalization. Left untreated, malaria can be fatal. According to the Centers for Disease Control and Prevention: --3.4 billion people live in areas at risk of malaria transmission in 106 countries and territories. --The World Health Organization estimates that in 2012, malaria caused 207 million clinical episodes, and 627,000 deaths. --About 1,500 cases of malaria are diagnosed in the United States annually, mostly in returned travelers. Dr. Phil Seidenberg, who spent five years living and working in Zambia as Global Rescue’s African Regional Medical Director, has treated many malaria patients in the course of his career. Dr. Seidenberg points out that significant global progress has been made with malaria over the past decade, with better control of malaria and fewer deaths from malaria for multiple reasons. We spoke with Dr. Seidenberg and posed five common questions that travelers may have about the risks, prevention and treatment of malaria. 1. How do I know if malaria is an issue where I’m traveling? For updated information on countries with malaria, use the resources available through either the Center for Disease Control (CDC) or the World Health Organization (WHO). Both of these organizations have maps with malaria risk levels indicated by country, and for regions within countries as well. Global Rescue members can contact Global Rescue for specific malaria advice. Travelers headed to Africa should be aware that, while progress has been made in controlling malaria on the continent, an estimated 91% of deaths from malaria in 2010 were in the African Region (CDC). According to the WHO, in recent years, four countries have been certified by WHO as having eliminated malaria: the United Arab Emirates (2007), Morocco (2010), Turkmenistan (2010), and Armenia (2011). It is important to consider the time of year of your travel. If a country has malaria, there is usually some seasonality to it. Typically malaria follows the rainy season, and is particularly active in the middle to the late part of the rainy season when water is pooling in areas; standing water allows malaria-carrying mosquito larva to populate. Another consideration is how rural will your travel be, because in general malaria is more common in rural areas. In locations around the world where there is greater control, such as in capital cities, travelers will likely face less risk. However, if travelers are planning on rural travel and there is malaria in these countries, they need to be well informed and take preventive measures. 2. Who are the people greatest at risk? Anyone who is not native to an area certainly faces an increased susceptibility to malaria. There is a level of tolerance that develops over time in those who are born and live in areas with malaria. A look at global statistics shows that greater than 75% of people who die from malaria are kids under five years old. If you are thinking of bringing kids along to areas with malaria, it is not a definite no-no but it is something to weigh carefully because the kids are the ones who do more poorly. The elderly are the next at-risk population, and the third class of traveler at an increased risk is pregnant women. 3. If I go to a malarial area, should I take medication? There are anti-malarial prophylactic medications (preventative therapies) that one can take. It is important to note, however, that none of these treatments is 100 percent effective. You should seek advice from your regular healthcare provider, or a provider experienced in travel medicine to help decide which of these medications might be best for your individual health profile. The primary recommendation I usually give is to choose a simple option such as Doxycycline, which is available everywhere. It needs to be taken only one to two days prior to travel, and the dose is just 100 milligrams once a day. It is contraindicated for kids younger than eight, mainly for cosmetic reasons because it stains teeth. Doxycycline is not a first choice medication for pregnant women, but may be okay to use during pregnancy in certain situations. The major side effect with its use is sun sensitivity. It causes a small number of people to burn really quickly and often the locations with malaria are sunny and tropical. Doxycyline can also be used for skin infections and, among other things, as treatment for some types of pneumonia, so it is in many ways useful to have in a travel case. Malarone is another great option. It is a very good, safe medication and very well-tolerated, although a little bit more difficult to find outside of travel clinics. Malarone is taken daily, and needs to be started only one to two days before travel. Side effects are minimal. Importantly, Malarone consists of a two-drug punch that greatly reduces the chance of contracting a resistant malarial strain. This medication cannot be used by pregnant women. Malarone is more expensive than the other options, and since it is taken daily, cost could be a factor for some, especially on longer trips. A third option is mefloquine, or Lariam. It is preferred by some people because it is taken on a weekly, not daily, basis. Lariam, which is safe for pregnant women, must be started at least two to three weeks before travel, and continued for up to four weeks upon completion of travel. While it is less expensive than some other options, Lariam has been shown to have more side effects than any other anti-malarial drug. However, many travelers use Lariam and are just fine. People always ask about Lariam because they hear about people reporting crazy dreams. Psychotic side effects are anecdotal, never really proven, but there is enough anecdotal evidence that typically I suggest other options first. 4. Are there other steps I can take or products to help protect against malaria? Definitely. Take precautions such as wearing long sleeves, using DEET repellants to ward off mosquitoes, and sleeping under netting. Most countries typically have mosquito nets in stores and even supermarkets, but if you’re concerned that you won’t be able to find them, it is a good idea to buy them in advance. The insecticide treated nets are really the ones to use. People sometimes pre-treat their clothing, too. It is important to know that the two peaks for malaria transmission are right at dusk and then right before sunrise. These are times when the mosquitoes are a little bit more active and more people are in contact with active mosquitoes, which is probably why transmission occurs most frequently between those two periods. Be especially cautious at these times. 5. What do I do if I’m traveling and I think that I may have malaria? The first step is to determine if you have malaria. In most African capital cities, you can go into almost any pharmacy and pick up a Rapid Diagnostic Test (RDT). It involves a simple finger prick, a few drops of blood, and a 15-minute wait for results. RDTs are part of the reason that malaria is under control, because we are no longer indiscriminately treating kids and people with fevers that are not malaria. Be cautious about the expiration dates, however, and do not buy anything that has expired. The RDTs are no different for kids versus adults. Another option is to go to a clinic. Almost any clinic operating in malarial countries will be able to do a very quick blood smear or a Rapid Diagnostics Test, too. What do you do if you have malaria? Most hospitals in malarial countries are more than capable of diagnosing and treating malaria. For treatment, the WHO recommends Artemisinin Combination Therapy, or ACT. However, do not assume that ACT is necessarily what you will receive. Absolutely ask for ACT by name. Most healthcare providers should know what that means, even though there are different trade names in some parts of the world. It is worth knowing that for almost all simple malaria, even complicated malaria, artemisinin compounds are the ones to use. Those that only have single artemisinin are, over time, quite bad for our malaria treatment options because the parasite develops resistance early. (Emerging artemisinin resistance is a major concern, according to the WHO, in certain areas of the world.) The combination therapy hits the parasite with two active medications working against it. For severe malaria, usually defined by altered mental status or organ dysfunction, in some places they are starting to do artemisinin IV drips. This approach has been shown to be better than good old quinine, which still is very effective. But typically if someone were hospitalized with severe malaria, quinine versus artesunate are the only real options for treatment. It is extremely important to be vigilant upon returning home. First, if travelers are taking a prophylactic that requires them to continue to take it for a few weeks afterwards, they must make sure to do that. Second, and even more dangerous in my view, is that it is hard to get malaria diagnosed in the States unless someone really thinks about it. In fact, this happened to friends of mine when they came back with their kids from Africa. It is an easy thing for a lab to take a look at a blood smear under with a microscope, but when medical professionals don’t ever see malaria that often, they’re not going to think about it. So, if someone comes back, gets sick and they’re worried about malaria, they need to really be careful that they tell whoever is seeing them, “By the way, I was in Haiti. Can you check me for malaria?” It could be a couple of months before travelers should consider themselves no longer at risk after returning home. Again, it is always a good idea for travelers to check in with their primary care provider or a travel medicine professional before traveling for a detailed discussion of their risk for malaria. | ||
|
| One of Us |
Great information. The RDT kits are great especially if you are trying to determine if you have malaria or something else like tick bite fever. I've used the RDT kits twice and "thankfully" both times was TBF - which still sucks. As far as prophylactics are concerned, I still like Lariam because you have amazing dreams (bonus) but Malarone seems to work well. The important consideration with any anti-malaria prophylactic is to seek immediate medical attention if you start to have joint pain, fever, or any non-specific problems after visiting a malaria area - regardless what anti-malarial you are taking. And you hope that you never encounter any form of Cerebral Malaria. No Bueno. ___________________ Just Remember, We ALL Told You So. | |||
|
| One of Us |
Touch off topic. Just got word from a friend his son was bit by a tick early last summer. Got sick, ten days in the hosp before they asked what it could have been. By then, his internals were badly damaged. A 28yr old guy healthy as could be til then is now barely able to feed himself or get around on a walker. Dr's say it's permanent. Take care of those bug bites folks! George "Gun Control is NOT about Guns' "It's about Control!!" Join the NRA today!" LM: NRA, DAV, George L. Dwight | |||
|
| One of Us |
TBF is fairly common and is basically like the flu on steroids for 8 to 10 days. It should be suspected anytime you begin to have muscle aches and fever. The lesser version of the infection is easily treated with either tetra or doxycycline. It is a good idea to travel with one or the other. As you are exposed "supposedly", subsequent reactions are milder and milder. I sure couldn't tell the difference the second time I got it. There is a more sever version and it can do exactly what you described - multi-organ damage and/or failure. No bueno. The bottom line, it is best not to tough-it-out when it comes to illness in Africa and Scotch is not a cure; I know... ___________________ Just Remember, We ALL Told You So. | |||
|
| One of Us |
Great information for all of us. G.R., welcome to Accurate Reloading! Thanks for joining our forums and we're looking forward to your future contributions. | |||
|
| One of Us |
Some of the best and most useful information I have read on this subject. Thanks. Mike Wilderness is my cathedral, and hunting is my prayer. | |||
|
| One of Us |
Thanks for your feedback. It is great to hear that the information provided is helpful and informative as you prepare for your hunt. Hope to hear from you all soon. | |||
|
| One of Us |
Can we buy the RDT kits in the US? If so, any suggestions on where? Thanks Larry Sellers | |||
|
| One of Us |
The are easy to obtain in RSA, but not sure about the US. We really see so little malaria in this country, then again, that's why so many doctors here miss-diagnose it and TBF. ___________________ Just Remember, We ALL Told You So. | |||
|
| One of Us |
http://www.alere.com/content/d...0Pan%20-%20A1795.pdf I found this here in NZ & Australia. Spoke to them. Made in Australia & easily available. They supply labs & hospitals. They have single test kits and 5 test kits. The 5 test kit costs $80 (US$65). "When the wind stops....start rowing. When the wind starts, get the sail up quick." | |||
|
| One of Us |
Super useful info, thanks for posting. | |||
|
| One of Us |
Larry - I have looked in the past and just did a quick search again. I cannot find them to be available here in the USA. Check CDC site for additional info regarding the kits. Mike ______________ DSC DRSS (again) SCI Life NRA Life Sables Life Mzuri IPHA "To be a Marine is enough." | |||
|
| one of us |
Related - my previous posts about Lyme Disease - Doxycycline is the standard treatment .Two weeks treatment at the hospital was not enough as all whom I met said. I'm now going through a second treatment . Now though ,I know a whole lot more about Lyme !! I've just found a doctor who's been treating Lyme patients for ten years .That's a RARE find. Lyme is nasty , take it seriously ! | |||
|
| One of Us |
This thread is certainly a keeper for the archives. Thanks everyone foe the time to share this and everyone's input! | |||
|
| One of Us |
Most people don't realize how prevalent malaria was in parts of the USA. The US no longer has that problem today because of widespread applications of DDT.  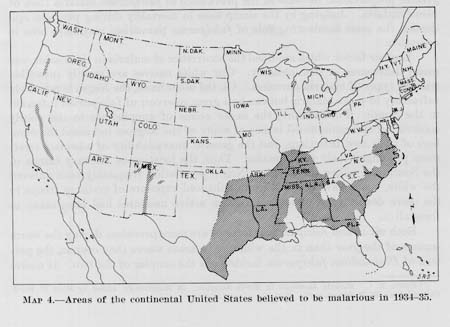
If liberal and widespread use of DDT was allowed today, malaria would be virtually eliminated throughout the world. Sadly, many hundreds of thousands of people die every year because brainwashed and misinformed environmentalists insisted on restricting or banning the use of DDT. Only recently, after public outcry and political pressure, has the use of DDT seen an increase in some of the most malaria infected regions of the world.
. | |||
|
| One of Us |
Mike - I checked lots of places on the net as well with no results. Several places have them, then state they cannot be sold in the USA. Seems funny something as simple and useful as these kits can't be purchased here? If anyone comes up with a USA source please contact me by PM or post here for all to see. Thanks. Larry Sellers SCI(International)Life Member Sabatti 'trash' Double Shooter R8 Blaser DRSS
| |||
|
| One of Us |
You can find them here - Rapid Test and here - Per 100 There are several different types of RDT kits so it is generally best to obtain them in the country where you may be exposed. ___________________ Just Remember, We ALL Told You So. | |||
|
| One of Us |
Thanks Opus - Checked it out and you can get a kit with 9each tests for $46.00 plus shipping. Sounds like just what I need. Will take this to Moz and most likely leave it with my PH for use in camp. To make an accurate diagnosis of Malaria in the bush seems like a good thing to be able to do? If positive, appropriate measures can go forward without any time lapse. Larry Sellers SCI(International)Life Member Sabatti 'trash' Double Shooter R8 Blaser DRSS | |||
|
| One of Us |
Larry, remember that symptoms generally appear 10 to 15 days after an infected mosquito bite. Typically, most travelers are home when then start to demonstrate parasitic infection. Unless of course you have the cerebral version, which happens much quicker and many times with fatal results. ___________________ Just Remember, We ALL Told You So. | |||
|
| One of Us |
Opus - Thanks for the additional info. I will be in Moz for at least 30 days plus the trip back home. I'll bring a couple test kits home with me just in case something shows up on return. Larry Sellers SCI(International)Life Member Sabatti 'trash' Double Shooter R8 Blaser DRSS
| |||
|
| One of Us |
Larry - Go to the Alere website: www.alere.com Doesn't sound to me like this product is the actual test but rather a means to certify the test. Also requires deionized water to reconstitute and storage between 35-45F degrees. I didn't read it all, but don't think it will work for us. Looks like the actual test kit sells for $600 for 12. Mike ______________ DSC DRSS (again) SCI Life NRA Life Sables Life Mzuri IPHA "To be a Marine is enough." | |||
|
| one of us |
I agree, this would appear to be the "rapid test" http://www.alere.com/us/en/pro...inaxnow-malaria.html BinaxNOW Brochure | |||
|
| One of Us |
In todays world the mosquito is still the most dangerous species that ever survived on this planet. 700,000 people die every year from malaria - in a world of modern medicine I have read where more people since the beginning of mankind have died from malaria than all other causes combined. I don't have the facts to back that up but if you think about it it sounds pretty reasonable | |||
|
| One of Us |
Heading to Zim in June, is there a consensus on AR members as to what they take? Wondering between Doxy and Malorone(sp?) | |||
|
| One of Us |
Doxy can result in sunburn but also works for tick bite fever. Good idea to have some along in your kit. Malarone is most commonly used anti-malarial and I switched to it from Larium some years ago - less side effects. Both Doxy and Malarone require daily administration. Good luck on your trip. Where in CA are you located? Mike ______________ DSC DRSS (again) SCI Life NRA Life Sables Life Mzuri IPHA "To be a Marine is enough." | |||
|
| One of Us |
Southern Cal, that great location for hunters and firearms aficionados. | |||
|
| One of Us |
nowhere in CA is a great location for hunters/shooters. i finish my last course of Doxy( from my Cameroon hunt) in 5 days. i start the next course in 29 days( just prior to leaving for the Caprivi)...i just prefer the extra protection offered for tick bite fever. Vote Trump- Putin’s best friend… To quote a former AND CURRENT Trumpiteer - DUMP TRUMP | |||
|
| One of Us |
If I was heading into communal land or and cattle country that has higher populations of Tick then I would use the Doxi or one of the generic versions of this antibiotic. If going some where like one of the lower Zambezi Safari areas I would use Malarone. | |||
|
| One of Us |
I'm headed to Mozambique Niassa reserve in September. What would be the consensus on what to take for this area?? Thanks, 163bc | |||
|
| One of Us |
Rachel Carson the author of Silent Spring should be equated to a mass murderer | |||
|
one of us |
Thanks for this very informative article Malaria diagnostic is part of my job.. Prophylaxywise Please IMPERATIVELY check out on a regular basis the CDC website. Malaria Information and Prophylaxis, by Country Drug resistances are constantly evolving, take no risks with partial recommandations. Strictly stick to the update CDC recommandations. What is accurate one day can be obsolete and dangerous next year. In some Asian countries it's better to use 2 drugs. 3 agents among 5 are prevalent in huntable African countries. Plasmodium falciparum can kill You, P vivax and ovale can relapse all your life long, no way to get cured. Prevalence, every subsaharian countries. Exceptions : THEORITICALLY RSA : only along the Zimbabwean border (Limpopo) Botswana :in the North Namibia : in the North PROTECTION : Protection against any insects and mites (ticks, spiders, ....) is a must. They transmit malaria, but also lots of virus, bacteria, protozoa and worms. Long sleeves, trousers and all your garments impregnated with insecticide/repulsive, DET creams, lotions or sprays, all are sound and healthy practices. Personally,even in countries where malaria is very rare, I am ever taking Lariam. Even in Tibet as one has to hop in China. Malaria diagnostic kit : available in most countries, if you can't find any, just ask your pharmacist, he can order some. If you scrupulously take your prophylaxy drug, there is no reason to check for malaria. A golden rule : any feverish people after a sojourn in Africa should be checked FIST for malaria, be it days, months, years, even 30 years later. J B de Runz Be careful when blindly following the masses ... generally the "m" is silent | |||
|
| One of Us |
I usually take Malarone even though there will be very few Mosquitoes at that time. I would also recommend carrying some Co-Artam or Arinate as a cure. | |||
|
| One of Us |
Not trying to be a wise ass here , just genuinely curious , but can malaria be spread by ticks and spiders ? I thought only the anopheles mosquito can transmit the parasite , and can the malaria parasite stay dormant in a human body for 30 years ? Maybe I'm reading this wrong. | |||
|
| One of Us |
i wondered about that too, Jan. as a physician, i was taught that only anopheles mosquitos transmitted malaria( at least that is what i was taught 35 years ago during a research project on malaria transmission in college). i guess things/knowledge have changed. and i never heard the part about the parasite staying dormant for 30 years before an acute case/outbreak. live and learn , i guess. Vote Trump- Putin’s best friend… To quote a former AND CURRENT Trumpiteer - DUMP TRUMP | |||
|
| one of us |
Sorry Jan and Jdollar I haven’t be clear. Only Anopheles are transmitting malaria, as Tse Tse fly sleeping sickness…etc. I am insisting on the fact that corporal and garment protections do protect against Arthropods ( insects, arachnids and mite), a formidable means to not get virus, bacteria, protozoa and worms Arthopod borne. A rule of the thumb, most often one agent transmit one disease , Plasmodium transmits malaria, Simulia fly the oncocerchosis… Other basic rules Malaria is little prevalent in large cities as for example Bangkok or Harare. Don’t take any risk, take your drug anyway. Hundreds of people get Arthropod borne diseases in and around airports in any country. Spraying the cabin in a plane isn’t sufficient. Passengers may and do release mosquitos and flies when opening their luggage or pouches in the arrival airport. I dearly attest that. Don’t attend airports without valid reason.
Some cases of Plasmadium vivax were dormant till 30 years. ..............or the patients were attending airports J B de Runz Be careful when blindly following the masses ... generally the "m" is silent | |||
|
| One of Us |
Thanks for clarifying . | |||
|
| Powered by Social Strata |
| Please Wait. Your request is being processed... |
Hunting African Big Game Hunting

Visit our on-line store for AR Memorabilia